For further reading and reference, explore key publications and global initiatives that have contributed to the evolution and standardization of MSICS:
Evolution of extracapsular technique into Phaco and MSICS
Comparison of MSICS with Phaco for ease of understanding
Illustration of surgical steps with video files
Complications & Management
Relevance in the Western World
Assessment & Reflection
🎧 Listen to this section
Introduction To MSICS
An extracapsular cataract extraction technique with a self-sealing scleral tunnel incision, designed to deliver phaco-comparable outcomes with minimal instrumentation.
Nomenclature
SICS – Small Incision Cataract Surgery
STSICS – Scleral Tunnel Small Incision Cataract Surgery
Manual Phaco / Sutureless ECCE – early variants
MSICS – Manual Small Incision Cataract Surgery
🎧 Listen to this section
Evolution Of Extracapsular Technique
A Brief History of MSICS
Early cataract procedures documented in ancient India (Sushruta, 600 BC)
Couching practiced historically; still in use in parts of Africa
Modern ECCE established foundations for current cataract surgery
MSICS introduced in early 1990s (Blumenthal)
Refined & popularised in Asia & Africa (Ruit & colleagues)
Revolutionised high-volume, low-cost cataract care globally
Davis, Geetha. “The Evolution of Cataract Surgery.” Missouri medicine vol. 113,1 (2016): 58-62.
Omoti, A. E. (n.d.). Complications of traditional couching in a Nigerian local population. West African Journal of Medicine, 24(1), 7–9 https://doi-org.ezproxy.uthsc.edu/10.4314/wajm.v24i1.28153
Roy PN, Mehra KS, Deshpande PJ. Cataract surgery performed before 800 B.C. The British journal of ophthalmology. 1975;59(3):171. http://search.ebscohost.com.ezproxy.uthsc.edu/login.aspx?direct=true&db=cmedm&AN=1093567&site=eds-live. Accessed March 18, 2020.
🎧 Listen to this section
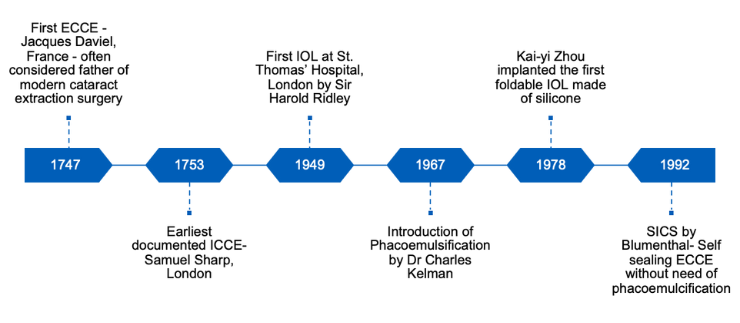
Landmarks In Cataract Surgery Advancement
🎧 Listen to this section
Davis, Geetha. “The Evolution of Cataract Surgery.” Missouri medicine vol. 113,1 (2016): 58-62.
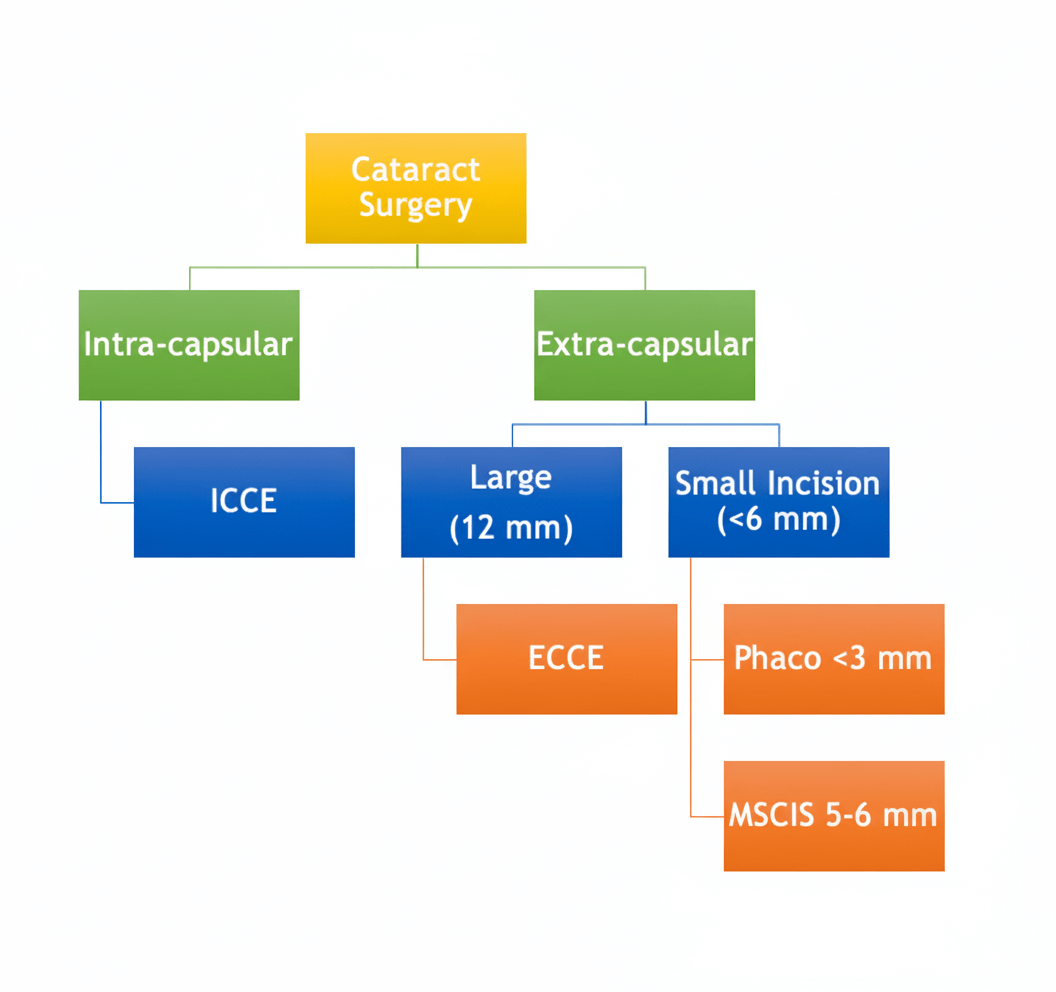
ICCE vs ECCE
🎧 Listen to this section
Indications Of MSICS
Mainstay of cataract surgery in developing world
Less costly and ideal for lower income settings
Short operating time
Minimum reliance on technology & instrumentation
Similar benefits of phacoemulcification
Rapid visual rehabilitation
Similar safety profile & Less astigmatism (than ECCE)
🎧 Listen to this section
MSICS vs. Phacoemulsification
Phacoemulsification
MSICS
Wound Construction– limbal or clear corneal
Conjunctival peritomy + SC tunnel construction
CCC + Hydro procedures
CCC + Hydro procedures
Nucleofractis
Nucleus Delivery
Cortical cleanup
Cortical cleanup
IOL implantation
IOL Implantation
Wound hydration
Wound closure
🎧 Listen to this section
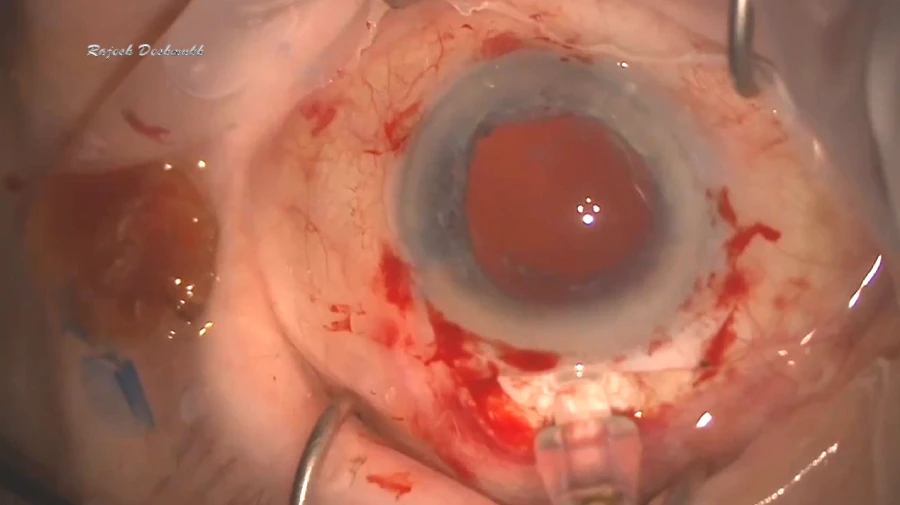
Step-by-Step Surgical Technique
Step 1: Wound Construction
Globe Stabilization – Secure the eye using a bridle suture
Conjunctival Peritomy – Create peritomy with Wescott scissors
Scleral Tunnel Creation – Form the tunnel with a crescent blade
Choose incision type:
Frown — preferred for stability
Straight with radial cuts — Bluementhal method
Prepare side pockets to support nucleus delivery
Entry into Anterior Chamber – Use a keratome to access the anterior chamber
🎧 Listen to this section
Wound Construction Continued…
Bridle Suture
The superior rectus bridle suture is used to stabilize the globe and optimize exposure during surgery.
This step allows controlled rotation and tension, preparing the eye for peritomy and tunnel construction.
4-0 silk suture passed through or beneath the superior rectus muscle, 8–10 mm behind the limbus
Tightening turns the globe downward
Provides controlled manipulation throughout the procedure
Peritomy and Hemostasis
Once the globe is stabilized, conjunctival peritomy exposes the sclera for tunnel construction.
Hemostasis is critical to maintain a clear surgical field and reduce intraoperative bleeding.
Conjunctival peritomy performed with Wescott scissors
Hemostasis achieved with cautery or pressure
Prepares the sclera for precise sclerocorneal tunnel formation
🎧 Listen to this section
Wound Construction Continued…
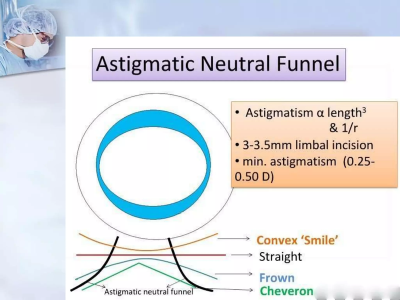
SC Tunnel Construction – Frown Incision
Self-sealing scleral tunnel is created to ensure smooth nucleus delivery and wound stability.
Three-planar tunnel: scleral, corneal, beveled AC entry
Perpendicular scleral incision 1/3–1/2 thickness, 2 mm posterior to limbus, preferably frown-shaped
Horizontal dissection extending 1–1.5 mm into clear cornea
Trapezoid configuration: wider inner corneal opening than outer scleral incision
Side pockets created for self-sealing
Crescent blade kept flat on globe for uniform tunnel depth
Anterior Chamber Entry & Corneal Lip Extension
Careful entry into the anterior chamber completes the tunnel and prepares the eye for safe nucleus delivery.
Proper corneal lip extension ensures a self-sealing incision while maintaining chamber stability.
Advance keratome slowly through the tunnel, tilting downward
Create internal incision parallel to the limbus
Extend incision laterally to include side pockets
Forms a larger inner corneal lip for a self-sealing wound
🎧 Listen to this section
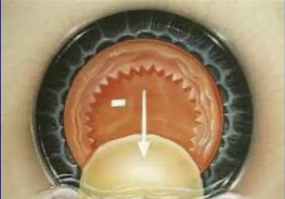
2. Nucleus Management
In MSICS, nucleus management involves prolapsing the nucleus into the anterior chamber and safely delivering it out of the eye.
Prolapse into Anterior Chamber
Use hydrodissection/hydroprocedures to loosen the nucleus
Employ a second instrument to rail out the nucleus
Bimanual techniques assist in safe manipulation
Nucleus Delivery
Viscoelastic-assisted delivery for controlled extraction
Blumenthal technique with anterior chamber maintainer
Instruments: Vectis or Fishhook to guide nucleus out
🎧 Listen to this section
Nucleus Management - Prolapse in AC
Hydroprocedures
Hydroprocedures, including hydrodissection and hydrodelineation, are performed to separate the nucleus from the cortex and capsule, ensuring safe mobility within the bag.
Once the nucleus is freely mobile, one pole is gently prolapsed into the anterior chamber under viscoelastic protection to safeguard the posterior capsule and corneal endothelium.
Involves hydrodissection (fluid wave beneath the anterior capsule) and hydrodelineation (separating nuclear layers).
Confirms free nucleus rotation before attempting prolapse.
Viscoelastic injected to protect both posterior capsule and corneal endothelium.
Properly sized capsulorhexis and deep anterior chamber are essential.
Avoid excessive fluid pressure to prevent posterior capsule rupture.
If hydroprocedures fail, proceed with Mechanical Prolapse techniques.
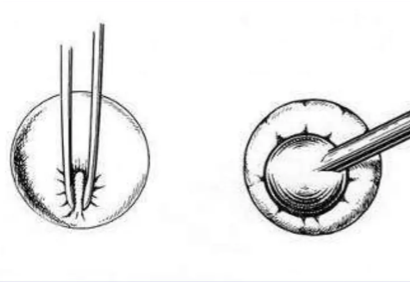
Mechanical Prolapse
When hydroprocedures alone are insufficient, the nucleus can be prolapsed mechanically using specialized instruments.
This technique is particularly useful in cases with a small pupil or difficult hydrodissection.
Use a Sinskey hook, cystitome, or bimanual technique (Sinskey + spatula)
Carefully manipulate the nucleus into the anterior chamber
Requires a properly sized capsulorhexis and deep anterior chamber
Ensures safe prolapse while protecting the posterior capsule and corneal endothelium
🎧 Listen to this section
Nucleus Management -Nucleus Delivery
Irrigating Vectis & Viscoexpression
Several techniques allow safe nucleus delivery while maintaining anterior chamber stability and protecting intraocular structures.
Irrigating Vectis: BSS-filled syringe introduced under the nucleus with viscoelastic cover; synchronized movements of bridle suture, Vectis, and hydrostatic jet guide nucleus out
Viscoexpression: Inject viscoelastic below the nucleus at 6 o’clock; create positive AC pressure while depressing posterior scleral lip
Both techniques ensure controlled delivery and protection of corneal endothelium and posterior capsule
AC Maintainer (Blumenthal)
Provides continuous positive pressure within the anterior chamber, ensuring a stable intraocular environment during nucleus extraction.
Uses an anterior chamber maintainer to maintain constant irrigation.
Enables controlled manipulation of the nucleus without chamber collapse.
Particularly useful in dense or mobile nuclei where chamber stability is crucial.
Fishhook
Offers a mechanical alternative for nucleus extraction using a simple, effective instrument modification.
A bent 30G needle is fashioned into a “fishhook.”
The hook is gently inserted beneath the nucleus under viscoelastic protection.
Allows precise engagement and controlled extraction of the nucleus through the tunnel.
🎧 Listen to this section
IOL Implantation – Through SC Tunnel
Foldable IOL Implantation
Foldable IOLs can be implanted smoothly through the sclerocorneal tunnel, making the procedure straightforward even with larger wounds.
SC tunnel provides adequate access for foldable lenses
Viscoelastic protects the corneal endothelium and anterior chamber
Technique is suitable for primary and secondary IOL implantation
PMMA IOL Implantation
Sclerocorneal tunnels are particularly suitable for rigid PMMA IOLs, often used in resource-limited settings or secondary procedures.
Allows implantation of PMMA lenses during primary surgery
Can also accommodate secondary IOLs, e.g., AC IOLs or iris-clipped lenses
Maintains anterior chamber stability and safe positioning of the lens
🎧 Listen to this section
3. Wound Closure
Proper wound closure ensures anterior chamber stability and minimizes surgically induced astigmatism, while maintaining the safety of the sclerocorneal tunnel.
SC Tunnel
Usually self-sealing if corneal lip is adequate
Optional 10-0 nylon or vicryl suture for large or dense nucleus incisions
Conjunctival or Tenon capsule apposition via ballooning or small suture
Optional 9-0 vicryl for larger incisions
🎧 Listen to this section
Complications & Management
Intraoperative and postoperative complications in MSICS are uncommon in experienced hands, but thoughtful management is essential for optimal outcomes.
Tunnel-related issues: Premature entry or inadequate tunnel construction can result in iris prolapse, hyphema, or a wound that is not self-sealing. These are often linked to incorrect dissection planes or poor technique.
Posterior capsule rupture (PCR): May occur during nucleus delivery or aspiration, increasing the risk of vitreous loss. If the nucleus drops into the vitreous, prompt referral to a vitreoretinal specialist is required.
Corneal edema and induced astigmatism: Typically result from excessive intraocular manipulation or wound leakage, underscoring the importance of meticulous surgical steps.
Other rare complications: Include zonular dialysis, Descemet’s membrane detachment, endophthalmitis, and IOL malposition—each requiring specific recognition and intervention protocols.
With proper training, careful preoperative planning, and adherence to evidence-based technique, complication rates in MSICS remain low and visual outcomes excellent.
Complication
Cause
Prevention
Management
Tunnel Leak
Irregular dissection
Precise three-plane technique
Stromal hydration or suture
PCR
Zonular stress
Gentle hydrodissection
Anterior vitrectomy, sulcus IOL
Nucleus Drop
Uncontrolled delivery
Vectis support for hard nuclei
Pars plana vitrectomy - Ref to VR
Corneal Edema
Endothelial trauma
Viscoelastic protection
Topical steroids, hypertonics
Astigmatism
Large/incorrect incision
Frown design
Spectacle correction
MSICS in the Developed World: Technique & Training
Manual Small Incision Cataract Surgery (MSICS) is increasingly recognized across developed countries as a valuable, evidence-based complement to phacoemulsification—especially for complex and high-risk cases. There is a growing emphasis on integrating MSICS into training curricula, skill-transfer workshops, and academic collaborations.
Recognized as a complementary technique alongside phacoemulsification, not a replacement
Preferred for hyperdense cataracts, pseudoexfoliation, phacodonesis, and zonulopathies
Offers superior endothelial protection in rock-hard nuclei and challenging surgical scenarios
Combines the advantages of ECCE (complete nucleus delivery, simplicity) with the benefits of phaco (smaller incision, faster recovery)
Increasing adoption within fellowship and residency programs, surgical skills workshops, and global exchange initiatives
Ifantides C, Ross AG, and others (2023) ‘A formal MSICS curriculum for US ophthalmology residents: survey study,’ Ophthalmology. Available at: View (Accessed: 5 September 2025).
Bejjenki P, Gurnani B, Kaur K et al. (2022) ‘Impact of a formal manual small-incision cataract surgery curriculum in an American ophthalmology residency program’, Indian Journal of Ophthalmology. Available at: View (Accessed: 5 September 2025).
Yaïci R, et al. Training in cataract surgery in Spain: analysis of the results of a simulation-based course for manual small incision cataract surgery. J Cataract Refract Surg. 2024.
Riaz Y, de Silva SR, Evans JR. Manual small incision cataract surgery (MSICS) with posterior chamber intraocular lens versus phacoemulsification with posterior chamber intraocular lens for age-related cataract. Cochrane Database Syst Rev, 2103;10.
Gogate P, Optom JJ, Deshpande S, Naidoo K. Meta-analysis to Compare the Safety and Efficacy of Manual Small Incision Cataract Surgery and Phacoemulsification. Middle East Afr J Ophthalmol. 2015 Jul-Sep;22(3):362-9. doi: 10.4103/0974-9233.159763. PMID: 26180478; PMCID: PMC4502183.
Impact of a formal manual small-incision cataract surgery curriculum in an American ophthalmology residency program Ifantides, Cristos; SooHoo, Jeffrey R; Christopher, Karen L Indian Journal of Ophthalmology. 71(6):2474-2477, June 2023.
Khanna RC, Kaza S, Palamaner SSG, Sangwan VS. Comparative outcomes of manual small-incision cataract surgery and phacoemulsification performed by ophthalmology trainees in a tertiary eye care hospital in India: a retrospective cohort design. BMJ Open, 2012;2(5).
Kongsap P. Visual outcome of manual small-incision cataract surgery: comparison of modified Blumenthal and Ruit techniques. Int J Ophthalmol, 2011;4(1):62-5.
Blumenthal M, Ashkenazi I, Assia E, Cahane M. Ophthalmic Surg, 1992;23(10):699-701.
Gogate PM, Kulkarni SR, Krishnaiah S. Safety and efficacy of phacoemulsification compared with manual small-incision cataract surgery by a randomized controlled clinical trial: six-week results. Ophthalmol, 2005;112(5):869-74.
Haripriya A, Chang DF, Reena M, Shekhar M. Complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital. J Cataract Refract Surg, 2012;38(8):1360-9.
Lynds R, Hansen B, Blomquist PH, Mootha VV. Supervised resident manual small-incision cataract surgery outcomes at large urban United States residency training program. J Cataract Refract Surg. 2018 Jan;44(1):34-38. doi: 10.1016/j.jcrs.2017.09.032. PMID: 29502616.
Commentary: Impact of manual small-incision cataract surgery on outreach and training curriculum across the world Bejjenki, Priyanka; Gurnani, Bharat; Kaur, Kirandeep; Tejaswini, Antarvedi; Sinha, Aprajita; Venkatesh, Dharavath; Morya, Arvind K Indian Journal of Ophthalmology. 71(6):2478-2479, June 2023.
Final Assessment & Summary
In summary, this module has equipped you with a comprehensive foundation in Manual Small Incision Cataract Surgery (MSICS)—from its historical and global context to the intricate surgical steps, complication management, and wet lab readiness.
Key takeaways include:
The biomechanical superiority of scleral tunnel construction for wound stability and healing.
Adaptive techniques for safe and effective nucleus delivery in a wide range of surgical scenarios.
MSICS is a proven complementary technique, supported by an extensive evidence base from published meta-analyses and international comparative studies.
By emphasizing patient-centered outcomes, MSICS empowers you to deliver equitable, high-quality cataract care across diverse clinical settings.By emphasizing patient-centered outcomes, MSICS empowers you to deliver equitable, high-quality cataract care across diverse clinical settings.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}